International Website
US Website
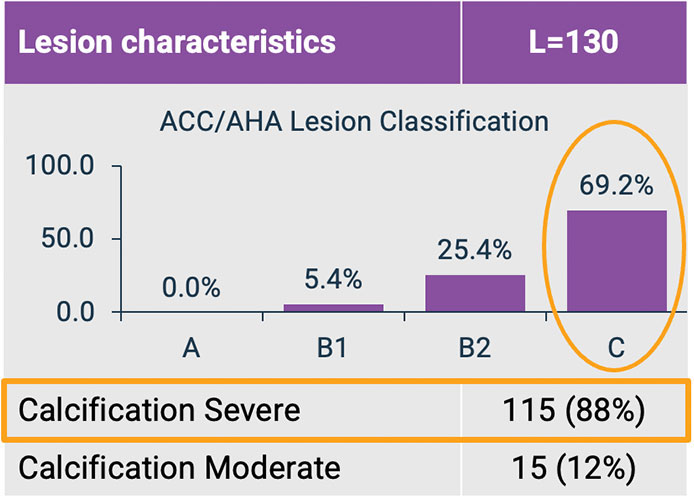
The MY-IVL clinical study was an investigator-sponsored post market study designed to assess the safety and performance of Hertz Contact Intravascular Lithotripsy (HC-IVL) to treat calcified, stenotic, coronary lesions prior to PCI in real-world practice. This all-comers study was comprised of complex patient population presenting with diverse calcium morphologies.
This clinical experience demonstrated HC-IVL is effective in modifying calcified coronary lesions across complex and high-risk patient populations. Imaging conducted in the study confirmed consistent plaque fracture and vessel expansion, supporting its use in challenging anatomies and lesion types.

§, Unstable angina, STEMI or NSTEMI.
‡, Stable angina or silent ischemia.
The MY-IVL Study outcomes demonstrated effective and safe fragmentation of diverse, severely calcified lesion morphologies in a complex all-comers patient population. HC-IVL provides a mechanical calcium modification approach designed to enable vessel expansion, while minimizing procedural complexity, particularly in high-risk and complex lesions.
(scroll horizontally to read entire table)
| Calcium Eccentricity | Eccentric Calcium | Concentric Calcium | Overall | |
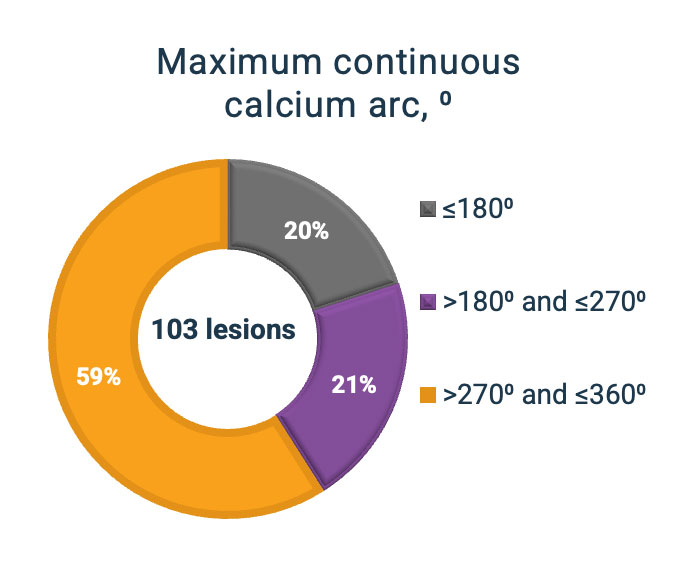
| Maximum continuous calcium arc, ° | ≤180° | >180° and ≤270° | >270° and ≤360° | |
Mean stent expansion‡, % |
123.15 ± 13.81(L=13) |
106.77 ± 18.30(L=13) |
110.96 ± 17.97(L=27) |
113.71 ± 17.80(L=58) |
‡Of the 58 lesions with mean stent expansion, 53 had baseline calcium arc available.
Imaging Core Lab adjudicated.
| Final Post-PCI | L=116 |
| Acute gain, mm | 1.75 ± 0.58 |
| Minimum lumen diameter, mm | 2.65 ± 0.56 |
In-lesion DS, % |
10.71 ± 11.49 |
In-lesion DS <50% |
116 (100.0%) |
In-lesion DS <30% |
109 (94.0%) |
Imaging Core Lab adjudicated.
*, One subject had perforation that occurred during stent deployment (not HC-IVL related).
**, No device related events were reported – Three cardiovascular deaths (CVDs) were assessed by the site as not related to the HC-IVL procedure; one death had unknown cause
Proportion of subjects with residual stenosis <30%, and without intra-procedural MACE
(Patients who received DES treatment post HC-IVL)
Minimum Stent Area‡ (MSA) for stented lesion after HC-IVL (Powered)
p <0.0001
(95% CI: 6.50-7.28)
Imaging Core Lab adjudicated. †, PG derived from the average MSA 5.65 ± 0.75 mm². ‡, OCT/IVUS measurements available: 94 lesions
*MACE defined as a composite of cardiovascular death, myocardial infarction and target vessel revascularization
**Performance Goal (PG) was derived from the average MSA (5.65 mm2) reported in prior IVL and RA studies1-3 with a statistical margin of 0.75 mm2
1Honton B, et al. ICARE trial, EuroPCR 2025
2Abdelhakim A, et al. CCI. 2022 Nov;100(6):979-989
3Ziad A, et al. Circ Interv. 2023, 16(10): e012898
Ready to break free from the limitations of console-based lithotripsy? Fill out the form and a representative will schedule a meeting as soon as possible.
In real-world practice, calcified coronary lesions rarely present in isolation or in ideal anatomy. Physicians are often treating patients with:
These factors make lesion preparation more difficult, limit device deliverability, and increase the risk of incomplete stent expansion.
The results of the MY-IVL investigator-initiated, all-comers study demonstrated real-world effectiveness in treating complex calcified coronary lesions.
The MY-IVL study observed HC-IVL treatment for 102 consecutive patients at a center, providing a real-world, all-comers analysis. Patients in the study included:
The MY-IVL study specifically evaluated this type of real-world population. The results demonstrated that calcium fragmentation can be performed safely and effectively with HC-IVL even in complex, high-risk cases.
Drug-eluting stents and bioadaptors rely on vessel compliance to expand properly and provide support for the diseased coronary artery in PCI. When calcium is rigid and unmodified:
Calcium fragmentation changes the mechanical properties of the lesion, allowing:
The MY-IVL study showed optimal levels of stent expansion were achieved across different calcium morphologies. The results confirmed the effectiveness of HC-IVL in coronary calcium modifcation.
Intravascular lithotripsy has emerged as a valuable tool for calcium modification. IVL is particularly useful in complex lesions where traditional approaches may be limited. In the MY-IVL study:
These results demonstrate that calcium fragmentation using IVL can support consistent procedural success, even in challenging real-world scenarios.
Yes, but this is one of the most difficult aspects of PCI. Patients often present with a mix of:
The MY-IVL study showed that calcium fragmentation using Hertz Contact IVL was effective across these diverse morphologies. Strong stent expansion outcomes were also observed regardless of calcium distribution.
Safety is a critical concern, particularly in complex patient populations.
In the MY-IVL study:
These findings support the use of HC-IVL as a safe approach to calcium modification in PCI, even with complex lesions and high-risk patients.
Lesion complexity directly influences:
In real-world PCI, physicians must adapt to:
Technologies that can perform consistently across these variables are particularly valuable in complex cases.
PMN 2504 Rev A
PMN 1777 Rev A